![]()
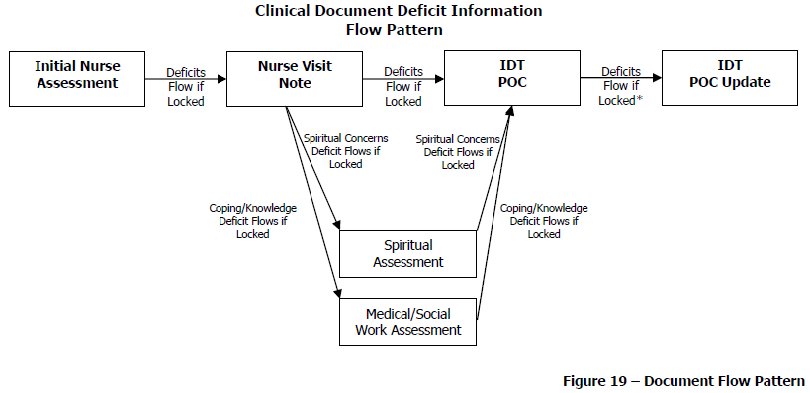
All deficits flow from the first locked document to the next document created, and so on, as long as each subsequent document created is locked.
The table below contains the complete list of hospice clinical documents in HEALTHCAREfirst :
Document Name |
Document Type |
Defaulting Flow Clinical Documents |
|
Initial Nurse Assessment |
Assessment |
P |
|
Medical Social Work Assessment |
Assessment |
P |
|
Spiritual Assessment |
Assessment |
P |
|
Discharge Summary |
Assessment |
|
|
Hospice Aide Care Plan |
Care Plan |
* |
|
Initial Plan of Care/Physician’s Orders |
Care Plan |
|
|
Palliative Performance Scale |
Care Plan |
|
|
IDT Plan of Care (POC) |
Care Plan |
P |
|
IDT Plan of Care (POC) Update |
Care Plan |
P |
|
Nursing Visit Note |
Visit Note |
P |
|
Hospice Aide Supervisory Visit Note |
Visit Note |
|
|
Hospice Aide Visit Note |
Visit Note |
|
|
Medical Social Work Visit Note |
Visit Note |
P |
|
Counselor Note |
Visit Note |
|
|
Spiritual Visit Note |
Visit Note |
P |
|
PRN Progress Note |
Visit Note |
P |
|
Telephone Progress Note |
Visit Note |
|
|
Medical Director Progress Note |
Visit Note |
|
|
Nurse Practitioner Progress Note |
Visit Note |
|
|
Physician Progress Note |
Visit Note |
|
|
Death Visit Note |
Visit Note |
|
|
Volunteer Visit Note |
Visit Note |
|
|
Inpatient Facility Rounds Visit Note |
Visit Note |
|
|
Imminent Status Review |
Supporting |
|
|
Fall Risk Screening (Multi-Factor) |
Supporting |
|
|
Braden Scale |
Supporting |
|
|
Case Communication |
Supporting |
P |
There are ten (10) clinical documents that participate in the document flow:
● Initial Nurse Assessment
● Nursing Visit Note
● IDT Plan of Care (POC)
● IDT Plan of Care (POC) Update
● Spiritual Assessment
● Medical Social Work Assessment
● Medical Social Work Visit Note
● Spiritual Visit Note
● PRN Progress Note
● Case Communication
* The Hospice Aide Care Plan flows to the Hospice Aide Visit Note. If the clinician indicates certain tasks to be performed by the aide on the care plan, the visit note flags those tasks as “to do” items so the aide knows specifically which tasks are to be performed. The Hospice Aide Visit Note displays two asterisks (**) next to the tasks that were indicated on the Hospice Aide Care Plan.
The remaining Defaulting Flow Clinical Documents are divided into two (2) categories:
The following table contains a comprehensive listing of the flowing deficits and the clinical documents in which they are found.
|
|
All deficits flow from the first locked document to the next document created, and so on, as long as each subsequent document created is locked. |
|
DEFAULTING FLOW CLINICAL DOCUMENT DEFICITS |
||||||||||
|
Deficits |
Comprehensive Documents |
Specialty Documents |
||||||||
|
Initial Nurse Assessment |
Nurse Visit Note |
IDT POC |
IDT POC Update |
Spiritual Assessment |
Spiritual Visit Note |
Medical Social Work Assessment |
Medical Social Work Visit Note |
PRN Progress Note |
Case Communication |
|
|
Cardiovascular |
P |
P |
P |
P |
|
|
|
|
|
|
|
Respiratory |
P |
P |
P |
P |
|
|
|
|
|
|
|
Physical Comfort/Pain |
P |
P |
P |
P |
|
|
|
|
|
|
|
Sleep |
P |
P |
P |
P |
|
|
|
|
|
|
|
Integument/Skin |
P |
P |
P |
P |
|
|
|
|
|
|
|
Wound 1 |
P |
P |
P |
P |
|
|
|
|
|
|
|
Wound 2 |
P |
P |
P |
P |
|
|
|
|
|
|
|
Wound 3 |
P |
P |
P |
P |
|
|
|
|
|
|
|
Wound 4 |
P |
P |
P |
P |
|
|
|
|
|
|
|
Elimination/Urinary |
P |
P |
P |
P |
|
|
|
|
|
|
|
Nutrition |
P |
P |
P |
P |
|
|
|
|
|
|
|
Musculoskeletal |
P |
P |
P |
P |
|
|
|
|
|
|
|
Neurological |
P |
P |
P |
P |
|
|
|
|
|
|
|
Gastrointestinal |
P |
P |
P |
P |
|
|
|
|
|
|
|
Endocrine |
P |
P |
P |
P |
|
|
|
|
|
|
|
Environmental Safety |
P |
P |
P |
P |
|
|
|
|
|
|
|
Grieving Anticipatory/ Bereavement Assessment ‡ |
P |
P |
P |
P |
|
|
P |
P |
|
|
|
Spiritual Concerns ‡ |
P |
P |
P |
P |
P |
P |
P |
P |
|
|
|
Coping/Knowledge ‡ |
P |
P |
P |
P |
|
|
P |
P |
|
|
|
Activities of Daily Living |
P |
P |
P |
P |
|
|
|
|
|
|
|
Coordination of Care |
P |
P |
P |
P |
P |
P |
P |
P |
P |
P |
‡ Depending on your processes, these areas may be controlled by MSW or Spiritual documents only, and editing the care planning items (problems, interventions, and goals) may be prevented in nursing documents. When completing nursing documents in this situation, clinicians can use the Coordination of Care page to communicate visit observations and suggest care plan updates for these areas.
Clinical Document Flow Example