The Discipline Codes Reference File should be modified only during the initial setup of Enterprise Edition with assistance from a HEALTHCAREfirst trainer. If you determine that any changes to this section are necessary after you have begun using Enterprise Edition, you must first contact Support for assistance. Changing the setup will disrupt data flow and can cause billing issues if not done correctly with assistance from the HEALTHCAREfirst team.
You should NOT, under any circumstances, change the visit behavior after initial setup. If you’re interested in making a change, contact the toll-free support line at 888-563-7016 to discuss it with a Support representative.
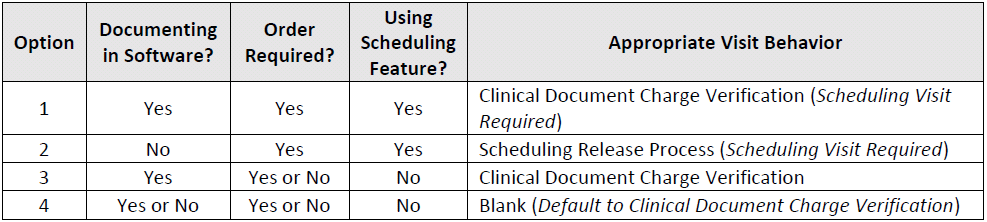
Depending on your agency setup, you may have some disciplines documenting in the system, some documenting on paper, some that will be using the Scheduling feature, some that won’t, and so on. There are different system settings available to accommodate each scenario, known as the Discipline Code Visit Behavior. There are four options for visit behavior, but only one option can be selected per discipline. The table below will help you determine which option to use for each discipline.
Select this option if staff for this discipline will fill out all clinical documentation within Enterprise Edition, generate orders, and schedule visits on the calendar that must fall within the frequency of the order.
Process flow for Option 1:
1. The Order is created.
2. Visits are generated to the calendar (to include a Visit Description and assigned Personnel, if known).
3. Clinician completes Visit and fills out all documentation in Enterprise Edition, which includes completing the P page.
4. The visit is Completed and Locked, which triggers the visit to be sent to Charge Verification.
5. Visit is released to Billing from Tools | Charge Verification.
6. Once released, the visit appears green on the calendar.
If for some reason part of your staff will not be following this process flow, a back office employee must add a PRN Progress Note to the patient chart with a reason code of “See Paper Chart” (this can be setup in the Reference Files). A custom form from Document Creator could also allow the back office staff to complete the P page. If your agency uses Electronic Signature you would then have the clinician Complete and Lock the document OR setup a signature of “See Paper Chart” for the back office staff. This is to allow the visit to be released to billing.
Select this option if staff for this discipline will NOT be filling out clinical documentation in Enterprise Edition, but will generate Orders and schedule Visits on the calendar that must fall within the frequency of the order.
Process flow for Option 2:
1. The Order is created.
2. Visits are generated to the calendar (to include a Visit Description and assigned Personnel, if known).
3. Clinician completes Visit and fills out all documentation on paper.
4. Documentation is turned in to back office staff and one of the following happens:
● Documentation is uploaded to the patient chart via Custom Documents
● OR documentation is kept on paper in a paper chart
5. Back office staff completes the Visit from the schedule, which causes it to display in tan on the calendar.
6. Visit is Released to Billing from Tools | Schedule Review.
7. Once Released, the Visit displays in green on the calendar.
Select this option if staff for this discipline will fill out all clinical documentation within Enterprise Edition and possibly generate Orders, but not schedule Visits on the calendar. This option requires you to manually review the chart to ensure all Visits fall within the appropriate frequency. This is not considered best practice.
Process flow for Option 3:
1. The Order is created. (This step is optional.)
2. Visits are NOT generated to the calendar.
3. Clinician completes Visit and fills out all documentation in Enterprise Edition, which includes completing the P page.
4. The Visit is Completed and Locked, which triggers the visit to be sent to Charge Verification.
5. Visit is Released to Billing from Tools | Charge Verification.
If for some reason part of your staff will not be following this process flow, they will need to manually key in the Charges/Visits to Accounts | Charge Entry (for Home Care) or Accounts | Productivity (for Hospice).
Select this option if staff for this discipline will have the choice of whether they want to complete documentation within Enterprise Edition or manually key in the Charges/Visits. Staff will not schedule Visits on the calendar with this option. This option requires you to manually review the chart to ensure all Visits fall within the appropriate frequency. This is not considered best practice.
Process flow for Option 4:
1. The Order is created. (This step is optional.)
2. Visits are NOT generated to the calendar.
3. Visits are entered in Enterprise Edition in one of three ways:
● Clinician completes Visit and fills out all documentation in Enterprise Edition, which includes completing the P page.
● OR Visits are manually keyed into Accounts | Charge Entry (for Hospice physician visits and/or Home Care visits)
● OR Visits are manually keyed into Accounts | Productivity (for Hospice)